Melanoma
Baseline tumor T cell receptor sequencing analysis and neo antigen load is associated with benefit in melanoma patients receiving sequential nivolumab and ipilimumab
Author: J. Weber
Abstract #1047O
Proffered Paper, Immunotherapy of Cancer
Friday, October 07, 2016, 4:45 – 5:00 p.m. CEST, Copenhagen
Overall survival and safety results from a phase 3 trial of ipilimumab at 3 mg/kg vs. 10 mg/kg in patients with metastatic melanoma
Author: P. Ascierto
Abstract #1106O
Proffered Paper, Melanoma and Other Skin Tumors
Saturday, October 8, 2016, 3:37 – 3:50 p.m. CEST, Copenhagen
Ipilimumab vs. placebo after complete resection of stage III melanoma: final overall survival results from the EORTC 18071 randomized, double-blind, phase 3 trial
Author: L. Eggermont
Abstract #LBA2_PR
Presidential Symposium 1
Saturday, October 8, 2016, 5:00 – 5:15 p.m. CEST, Copenhagen
Safety profile of nivolumab and ipilimumab combination therapy in patients with advanced melanoma
Author: M. Sznol
Abstract #1123P
Poster Session, Melanoma And Other Skin Tumors
Sunday, October 9, 2016, 1:00 – 2:00 p.m. CEST, Hall E
Safety of reduced infusion times for nivolumab plus ipilimumab and nivolumab alone in advanced melanoma
Author: S. Martin-Algarra
Abstract #1125P
Poster Session, Melanoma and Other Skin Tumors
Sunday, October 9, 2016, 1:00 – 2:00 p.m. CEST, Hall E
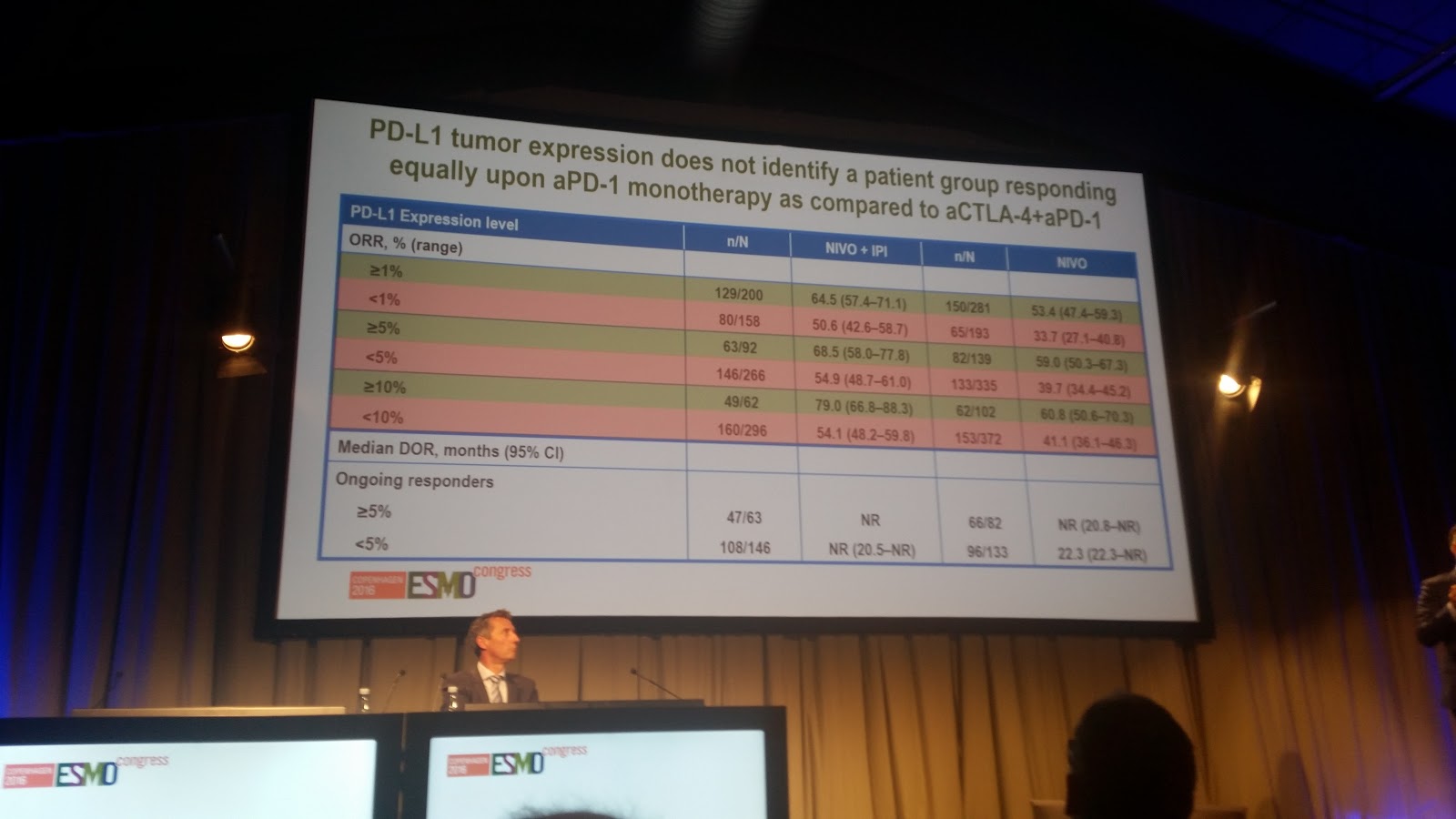
PD-L1 expression as a biomarker for nivolumab plus ipilimumab and nivolumab alone in advanced melanoma: A pooled analysis
Author: G. Long
Abstract #1112PD
Poster Discussion, Melanoma and Other Skin Tumors
Monday, October 10, 2016, 11:00 a.m. – 12:00 p.m. CEST (11:30 – 11:50 a.m. CEST),













































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}